

Healthy Liver: Bringing FibroScan into Mental Health Care
8th April 2026
Written by Majed Al Masri (Tower Hamlets Tobacco Dependency Advisor) with contributions from Vernanda Julien (Improvement Advisor)

The problem
People living with severe mental illness often face a double burden: the challenges of their mental health condition alongside a significantly higher risk of physical health problems. Among these, liver disease is particularly important. Factors such as long-term use of psychotropic medication, higher rates of smoking and substance use, poor diet, and reduced access to preventative healthcare all contribute to increased risk. Yet despite this, liver health screening is not routinely embedded within inpatient mental health care.
This gap formed the foundation of our QI project, Healthy Liver: Liver Scans for Inpatients with Severe Mental Illness, delivered in collaboration with Barts Health NHS Trust, with support from Sophie Livett (Lead Nurse in Hepatology, Royal London Hospital), Dr Peter Byrne (Consultant Liaison Psychiatrist, Royal London Hospital), and Ogechi Anokwuru (ELFT Trust Tobacco Dependency Lead).
Before the project began, FibroScans was not part of standard physical health checks within ELFT, meaning the baseline for liver screening was effectively 0%. The aim was to offer FibroScan liver health checks to 90% of eligible inpatients and complete the scan for 60% of patients who have been offered by March 2026.
Starting theory
We started with two acute inpatient wards in Tower Hamlets: Globe Ward for male patients and Roman Ward for female patients. A small but dedicated team delivered the project on the ground — myself as the QI lead, nurses Emily Brosnan-Guers and Jane Dalton performing the scans and explaining results, and a service user involved through Big I, supporting engagement by speaking to patients, building trust, and collecting feedback. This combination of clinical and lived-experience input proved essential in making the intervention acceptable and approachable.
Like many QI projects, the beginning was not without challenges. Governance requirements meant completing a Data Protection Impact Assessment (DPIA) and an Information Sharing Agreement (ISA) before starting. In addition, some staff initially expected to support the project were unable to do so due to rota changes. As a result, the work was carried forward by a small core team, with strong support from ward managers and nursing staff helping to keep the project moving.
To support the design of the project, a driver diagram (Figure 1) was developed to map out our teams theory of change which clearly defined the aim and key drivers of the project and a process map (Figure 2) was developed to map out the workflow of the intervention.
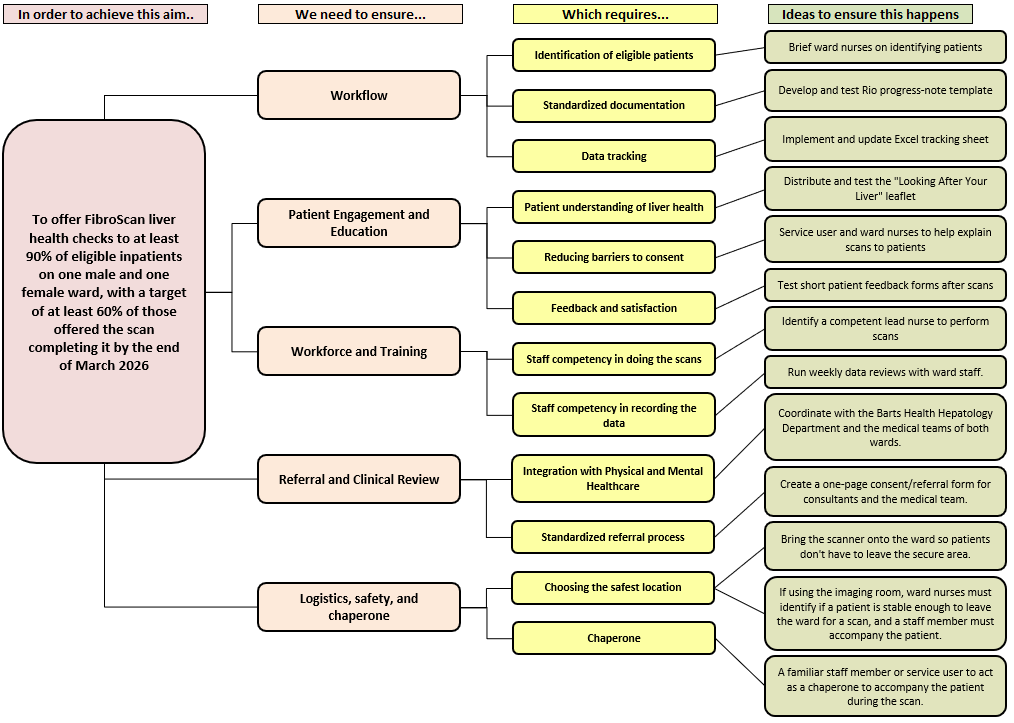
Figure 1. Driver Diagram – Offering FibroScan liver health checks to inpatients
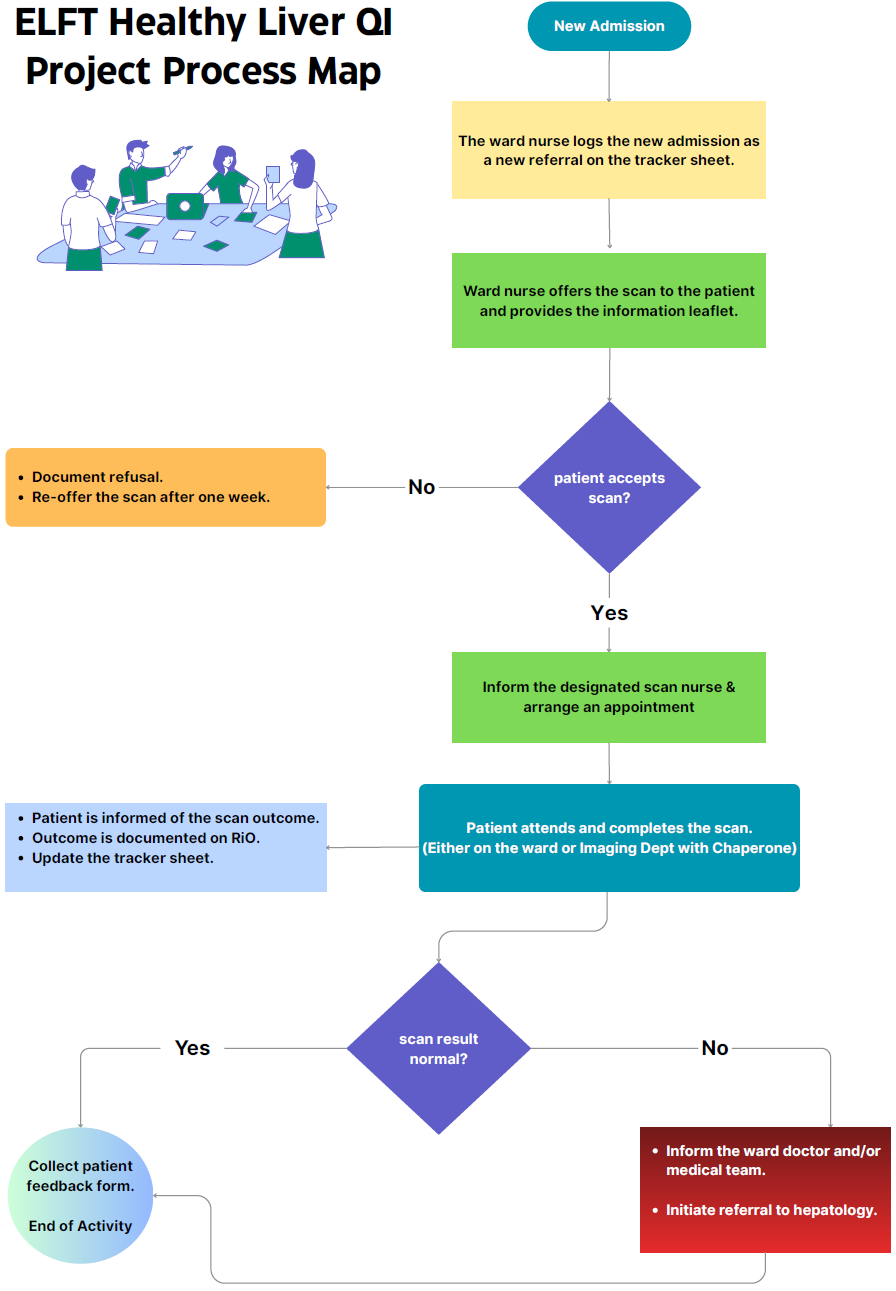
Figure 2. Health Liver process map
Testing changes
During the project we refined the process of identifying new admissions and offering the scan to patients. In the first cycle of testing, patients were identified, offered a FibroScan, and provided with a patient leaflet at the point of contact to support understanding of the scan. A service user was actively involved in supporting delivery, helping to offer the scan to patients and collecting feedback forms after the scan was completed. Due to staffing constraints, I took on a more active role in identifying patients and offering the scan to ensure continuity.
In a follow up PDSA cycle, staff members on the ward were encouraged to participate in the scans themselves and to be involved in offering them to patients. This helped to increase patients’ confidence and willingness to engage with the intervention. Additionally, it also supported greater staff engagement with the project and contributed to them feeling more confident when discussing the scans with patients.
Key learning and evidence of improvement
During the first phase of testing of the project on the acute wards, we saw strong engagement from patients. The majority were willing to take part in the scan, and the process proved feasible to deliver within the ward environment. However, as the data began to emerge, an important pattern became clear: most results were either normal or showed only mild abnormalities, such as fatty liver. This prompted a key question — were we targeting the right patient group to detect clinically significant disease?
To explore this, we introduced a PDSA cycle, expanding the project in weeks 6 to 8 to include Leadenhall, the older adults ward. This decision was based on the hypothesis that older patients may have a higher burden of undiagnosed liver disease, and therefore a greater likelihood of clinically meaningful findings.
This proved to be one of the most important learning points of the project. Over the final three weeks, 16 patients were scanned on Leadenhall ward, and 2 of them were found to have significant liver disease (fibrosis or cirrhosis) requiring referral to hepatology. This represents a 12.5% positive rate, which was notably higher than what we observed in the younger acute wards. It suggested that while the intervention was feasible across settings, its clinical impact would be greater when targeted appropriately.
Looking at the project as a whole, the overall engagement remained strong. Across the 8 weeks, 85 patients were included, all 85 patients were offered a scan (100%), and 72 (84.7%) patients completed it (Figure 3), exceeding the original target of 60%. Thirteen patients declined the scan (15.3%), which is expected in this setting and still reflects good overall uptake. Among completed scans, 61.1% were normal, 36.1% showed fatty liver, and 2.8% required referral due to liver stiffness. Importantly, the cases requiring referral were identified through the expansion to the older adult ward, reinforcing the value of the PDSA approach.
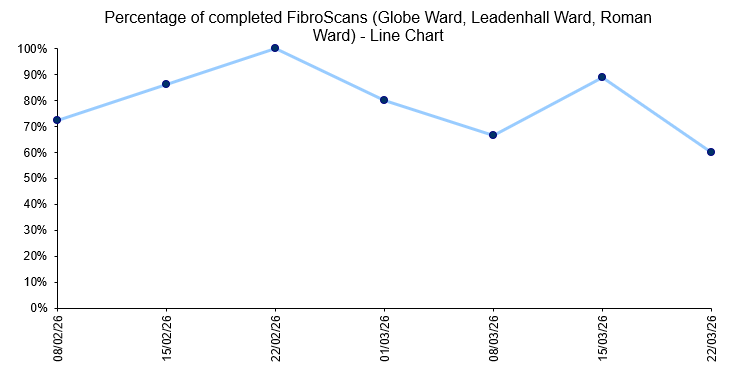
Figure 3. Line chart – Percentage of completed FibroScans in Globe Ward, Leadenhall Ward and Roman Ward
Patient and staff feedback
Patient and staff feedback formed an important balancing measure for this project. Feedback was collected from 51 participants across all wards. The results were highly positive, with 92% of respondents reporting that the scan was explained clearly, 80% finding the patient leaflet helpful, and 86% reporting a much better understanding of liver health following the intervention. In addition, 96% of patients felt comfortable and safe during the scan, and 76% reported feeling much more confident about how to look after their liver. Some of the feedback captured the impact more powerfully than numbers alone:
“I wouldn’t normally think about having a liver scan, but I thought to myself, why not.”
“I am grateful for Dr Majed to do this test on my liver today. My new me will be healthier.”
“Well appreciated as I have more knowledge on how to manage a healthy diet.”
“Very nice team… very friendly and approachable — keep up the good work.”
“Feeling very good, also found the process useful.”
Staff feedback was equally encouraging:
“The scan is very important and the scheme is quite interesting.”
“It has been an enjoyable, informative, and well explained session.”
These reflections highlight that the project was not only about detecting disease, but also about improving understanding, building trust, and supporting patients to think differently about their physical health.
Ending theory and next steps
As the project came to an end, we reached an important conclusion. Initially, the aim was to introduce liver screening across inpatient wards. However, through testing and learning, the project evolved to show that targeting specific populations, particularly older adults, leads to greater clinical impact. As a result, the service will continue on Leadenhall ward, where the need appears greatest. There is also growing interest from physical health teams in expanding this model to other wards and sites within ELFT.
This project has shown that improving physical healthcare in mental health settings is not just about introducing new interventions, but about continuously learning, adapting, and listening to both data and patient experience. It is a step towards more integrated, holistic care, where physical and mental health are addressed together rather than separately.
Learning through the Improvement Leaders’ Programme
This project was also part of my journey through the Improvement Leaders’ Programme, which played an important role in shaping how the work was designed and delivered. Through the programme, I developed key QI skills including building a driver diagram, mapping processes, and using PDSA cycles to guide improvement. The structured approach helped turn an initial idea into a practical and measurable intervention. I also received valuable support throughout the project from my QI coach, Paulina Marchewka, and my improvement advisor, Vernanda Julien, whose guidance was instrumental in maintaining direction, overcoming challenges, and supporting ongoing learning.
Most Read Stories
-
Why is Quality Control important?
18th July 2018

-
2016 QI Conference Poster Presentations
22nd March 2016
-
Recognising Racism: Using QI to Help Take Action
21st January 2021

-
QI Essentials: What does a Chief Quality Officer do?
18th March 2019

-
-
Using data enabled us to understand our problem
31st March 2023


Follow QI on social media
To keep up to date on the latest concerning QI at ELFT, follow us on our socials.
