

QI Essentials: Top down AND bottom up
17th October 2019
Deciding between a top-down approach to improvement and a bottom-up approach to improvement is a false – and meaningless – choice. We need to support both. It’s about top-down AND bottom-up, at the same time… Have a read of Amar’s latest QI Essentials Blog…
Should our quality improvement activity be directed at strategic areas of priority? Should we define, from the top of an organisation, what every team’s QI work should be aimed at?
But how does that fit with focusing on what matters most to those we serve, our patients and service users, and also what matters most to those in our point-of-care teams? How can we engage our teams in quality improvement without giving them the autonomy and power to define what they choose to work on?
Herein lies one of the big dilemmas in applying quality improvement work within a large complex organization. What I hope to describe in this blog is that deciding between a top-down approach to improvement, and a bottom-up approach to improvement, is a false, and meaningless, choice. We need to support both. It’s about top-down AND bottom-up, at the same time…

At East London NHS Foundation Trust, many people have described our quality improvement design as being largely bottom-up, akin to letting ‘a thousand flowers bloom’. And it’s true, to an extent. In the first year of our QI programme in 2014, we did support those who we were keen to be our early adopters to choose their own projects. But even in those early days, we had two high-level aims (reducing harm, and right care, right place, right time) to which all projects had to be aligned. They were loose aims, but there was some alignment to Trust strategy, even in those very early days.
We chose, though, to intentionally design our quality improvement to be as inclusive as possible. We didn’t want to just identify two or three big complex topics or areas for our improvement activity to focus on. We wanted everyone to feel that they could be part of this movement, and so we allowed a lot of scope for any and all projects to join. We valued engagement and interest above all else at this stage, realising that if we achieved enough energy in the first year this would become a real driving force for the future.
Within a year though, we had started to form some light-touch governance structures around our QI work so that projects now had to go through a locally-led approval process to ensure that teams were tackling topics that were meaningful. We also started to get much clearer about our high-level strategic improvement priorities.
Ultimately, if all our teams work on disparate topics, without any alignment around strategic priorities, all this improvement activity doesn’t really serve to move us in a common direction towards our mission as an organisation. For me, that’s akin to waste. So we do need to find a way to ensure that our improvement activity is aligned to high-level goals, but in a way that is shaped by what matters to those closest to where care is delivered.
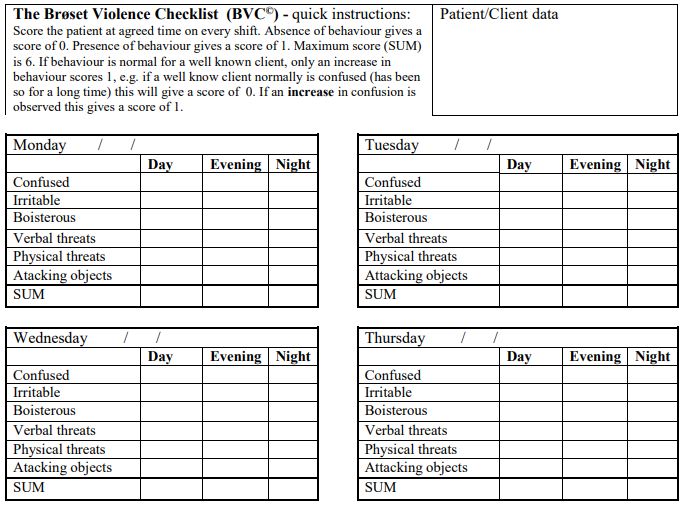
When we started to identify our high-level priorities, we realised pretty quickly that the assumption that what matters at Board-level and what matters at team-level are different is not necessarily true. Our data and conversations at the Board showed us that our number one safety issue was inpatient physical violence. But it also turned out that, given the opportunity, plenty of our inpatient wards chose to work on inpatient physical violence because it really mattered to them too. Access to services was a major issue for a lot of our service users, and it also turned out to be a big topic of interest for our Board and commissioners. So there’s perhaps an unrecognised level of synergy in priorities at both ends of an organisation. Priorities identified at the point of care often align naturally with priorities aligned at the most senior levels of the organisation.
The clearer we can make our strategic improvement priorities, and the better able we are to communicate why these are important, the more likely we are to engage our teams and service users to see how their work can align to these. Our leadership team spent a lot of time talking about our two ‘big dots’ of harm reduction and right care, right place, right time back in 2014. And we similarly reinforce our current four strategic priorities through lots of our formal and informal communications today at ELFT.

For me, the top-down / bottom-up debate is really about balance. We of course have to make sure that our improvement work is aligned to the strategic priorities for the organisation. If we don’t achieve this, then our quality improvement work will remain on the periphery – a ‘nice-to-do’ but not integral to the way the organisation functions and delivers for those it serves.
As with so much of our improvement work, it’s largely a question of how you do this in a careful, sensitive and thoughtful way. Having an open dialogue is a way into creating this fine balance between strategic priorities and point-of-care priorities. Given the opportunity to converse and discuss what really truly matters, and involving a range of people from all levels of an organisation, we often find that there isn’t as much divergence as we originally thought.
 Now, all our quality improvement work begins with a very simple question: What matters most? This question can be asked of everyone, no matter whether you’re at the Board, working in a clinical or corporate team, or receiving care as a service user. This helps bring clarity to both our strategic priorities, and our improvement priorities at team level. Around two-thirds of our quality improvement work at ELFT is now directly aligned to our four strategic objectives. But that still leaves a third that isn’t. For me, that’s a great asset and a real virtue in our approach to improvement at ELFT.
Now, all our quality improvement work begins with a very simple question: What matters most? This question can be asked of everyone, no matter whether you’re at the Board, working in a clinical or corporate team, or receiving care as a service user. This helps bring clarity to both our strategic priorities, and our improvement priorities at team level. Around two-thirds of our quality improvement work at ELFT is now directly aligned to our four strategic objectives. But that still leaves a third that isn’t. For me, that’s a great asset and a real virtue in our approach to improvement at ELFT.
Given the choice, I will always err on the side of giving teams of staff and service users the latitude to work on whatever they feel is the most important issue to tackle. Ultimately, without the will and ideas of those closest to the point of care, how would we improve at all?
You can read all past QI Essentials posts here.
Most Read Stories
-
Why is Quality Control important?
18th July 2018

-
2016 QI Conference Poster Presentations
22nd March 2016
-
Recognising Racism: Using QI to Help Take Action
21st January 2021

-
QI Essentials: What does a Chief Quality Officer do?
18th March 2019

-
Using data enabled us to understand our problem
31st March 2023

-

Follow QI on social media
To keep up to date on the latest concerning QI at ELFT, follow us on our socials.
