

Tower Hamlets Autism Service – Improving access for underrepresented populations
25th February 2025
Written by Emma Grisdale (Clinical Psychologist), Laura Humphries (Consultant Psychiatrist) and Vernanda Julien (Improvement Advisor)

Figure 1: Tower Hamlets Autism Service Team
Tower Hamlets Autism Service (THAS) have identified that we would like to improve access to our service by under-represented groups.
Background
We completed an audit of the RIO clinical record system between June 2024 to February 2025, in order to investigate the extent to which referrals to our service were representative of the population of Tower Hamlets. We hoped to identify any notable cohorts of excluded or under represented people.
We found that referrals received are not representative of the demographics of the local population, particularly with regards to ethnicity.
This inspired the idea for our newest QI project which we hope to align with the principles of the triple aim framework (e.g. reducing health inequalities and improving patient experience).
We found that Bangladeshi women are currently the most starkly under-represented group in relation to referrals to the service – 15% of female referrals were Bangladeshi women, whereas Bangladeshi women make up 34.6% of the female population of Tower Hamlets (Figure 2).
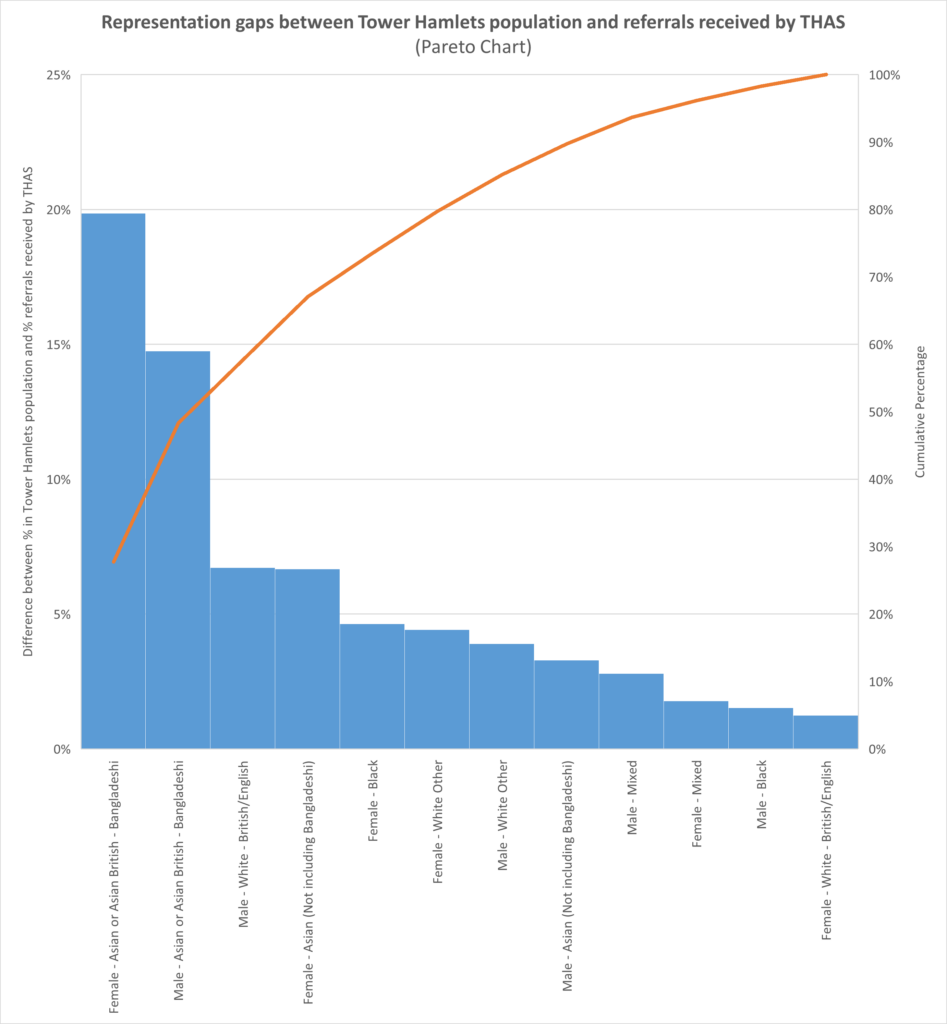
Figure 2: Pareto Chart showing the representation gap between Tower Hamlets Population and referrals received by THAS
Additional trends identified were that GPs were three times more likely to refer a White British woman than a Bengali woman and white British women were five times more likely to self-refer than British Bengali woman.
We aim to identify the reasons behind these discrepancies and locate potential barriers to accessing our service. Our improvement aim is to increase the percentage of referrals of Bangladeshi women to 30% by December 2025 in order to bring this more in line with the local population figure.
Why is it important?
Autistic individuals have increased risk of chronic physical and mental health conditions and ethnic minority groups generally have poorer health outcomes compared to the overall population.
We want to understand the inequalities in accessing our service to improve equity of access and outcomes for our service users.
Project team
Our project leads, Clinical Psychologist Dr Emma Grisdale and Consultant Psychiatrist Dr Laura Humphries joined the ELFT QI Improvement Leadership Programme (ILP) in October 2024 which has supported the work on the project.
The ILP has been a really useful opportunity to think through all of the different stages of planning the project and going about coming up with change ideas. Our understanding of the rationale behind the QI approach has developed and improved. It has allowed us to make sure that we have the right range of voices in the room to make up an effective project team. We have also learnt strategies to improve the process of chairing, managing and setting up the project.
Being part of the wider QI community has been a really valuable experience. Gaining others’ perspectives on our project and hearing about their projects has been invaluable. We are also very grateful for the support of our fantastic improvement advisor and project sponsor.
Our project team consists of Vernanda Julien (Improvement Advisor), Day Njovana (QI Sponsor), Laura Humphries (consultant psychiatrist, project lead), Emma Grisdale (clinical psychologist, project lead), Felicity Bowden (autism service operational lead), Nuala Murphy (occupational therapist), Josie Moriarty (support worker), Faaiza Ullah (service user), Zoe Thomas (trainee clinical psychologist), Sadiya Khanum (administrator), Gemma Nicholson (speech and language therapist), Jessie Atack (social worker), Alli Badasconyi (consultant psychiatrist) and Liz Higgins (occupational therapist).
Understanding the problem
We explored the possible factors contributing towards the low referrals of women of Bangladeshi background, using a fishbone diagram (Figure 3).
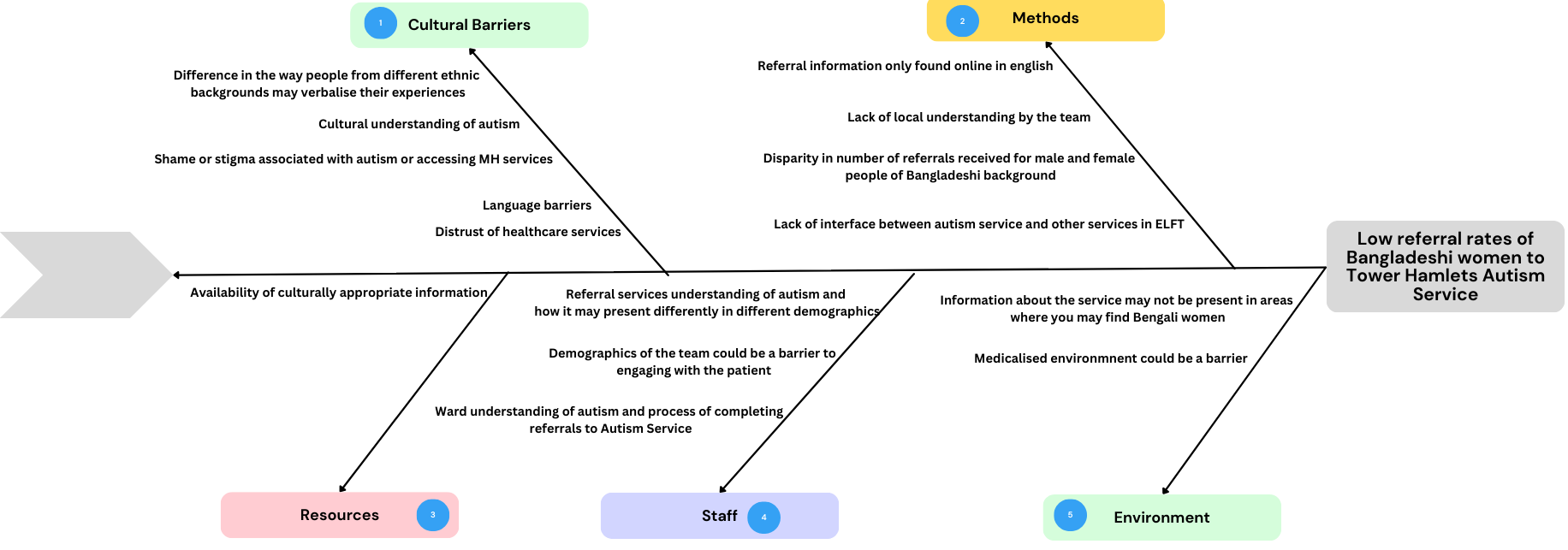
Figure 3: Fishbone Diagram – Low referral rates of Bangladeshi women
Our theory of change
Once we had an understanding of the problem, we went on to develop our theory of change using a driver diagram (Figure 4). This helped us to identify changes we could test which we believe could lead to an increase in referrals of Bangladeshi women.
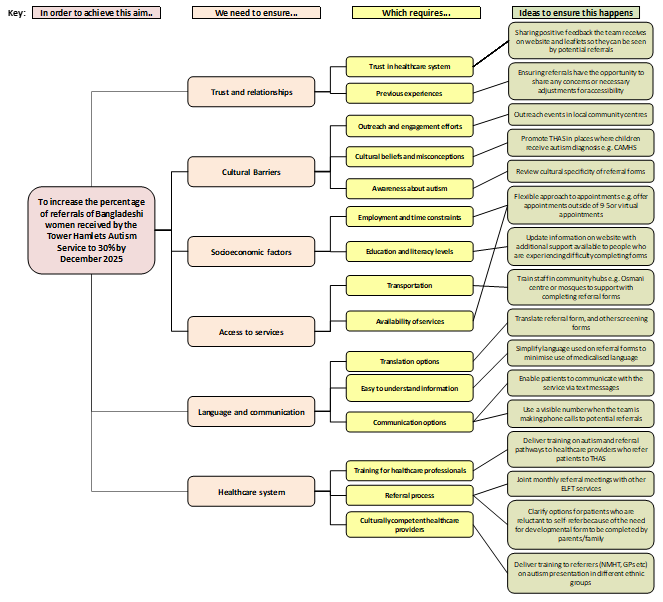
Figure 4: Driver Diagram – Increasing the percentage of referrals for Bangladeshi women
Testing changes and data collection
We have used multi-voting and structured discussions to prioritise the tests of change we would like to take forward. This has helped us to identify which tests of change would be our quick wins and our high impact changes.
Our first test of change will involve making changes to our website to ensure the information is easy to understand and translated information is easily available for non-English speakers.
We have collected baseline data on the percentage of referrals we have received for Bangladeshi women between June 2024 and February 2025 (Figure 4). We will continue to monitor this data as our outcome measure to determine the impact of our tests of change. We will also look at the number of self-referrals we receive as a process measure.
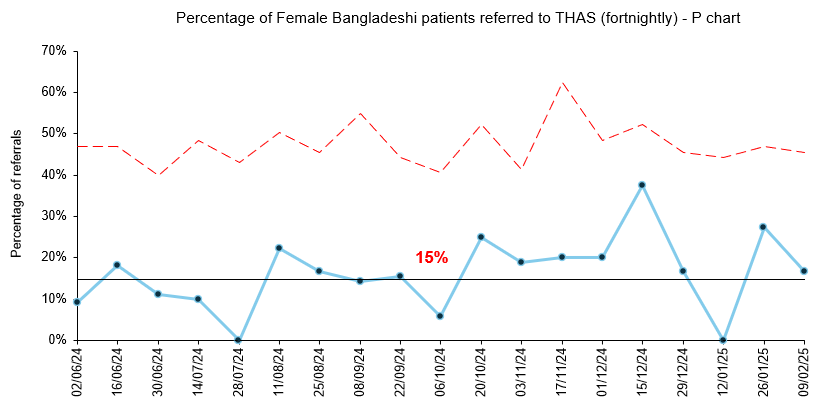
Figure 4: P Chart – Percentage of Bangladeshi women referred to THAS (baseline data)
Next steps
We believe our high impact changes will require strengthening our relationships with community centres which are regularly accessed by Bangladeshi women to raise awareness of autism and our service.
We also believe that increasing the cultural competence of referrers will strengthen their ability to recognise the ways autism may present in different ethnicities and genders.
We will begin planning the next phase of our tests of change and continue to collect quantitative and qualitative data to determine impact.
Most Read Stories
-
Why is Quality Control important?
18th July 2018

-
2016 QI Conference Poster Presentations
22nd March 2016
-
Recognising Racism: Using QI to Help Take Action
21st January 2021

-
QI Essentials: What does a Chief Quality Officer do?
18th March 2019

-
Using data enabled us to understand our problem
31st March 2023

-

Follow QI on social media
To keep up to date on the latest concerning QI at ELFT, follow us on our socials.
