

From Quality Improvement to Quality Control
22nd November 2016
By Auzewell Chitewe, Senior Quality Improvement Lead

Auz Chitewe – Senior QI Lead
An inevitable question a Quality Improvement (QI) project team will ask themselves at some point is: “When can we say we have achieved our aim and close our project as ‘complete’?”. Some projects close without achieving their aim because the initial aim is no longer achievable due to some significant change or understanding of the system the project was trying to effect. On the other hand, some projects close because they have achieved their aim. For these projects, the challenge is deciding when to close this project and the uncertainty of whether the gains can be sustained when there is no longer a dedicated project team working on this problem and reviewing the data regularly.
What would you conclude when you look at the chart in figure 1 for the period up to 25th June 2016? At what point within that period would you have made a decision to close the project as ‘complete’? The answer to that question is: “it depends”. One would have to engage with the subject matter experts, those directly involved or affected by the project. They will have some insights into whether the changes that have led to the improvement are embedded into the day-to-day activities for the ward and whether this is sustainable.
The chart (figure 1) taken from the Ivory ward project which had an aim to “Promote care in a less restrictive environment by reducing length of in-patient stay to less than 45 days and bed occupancy to less than 70%” on this functional older adults psychiatric ward. The team discussed closing the project in January 2016 but decided not to because they knew that some aspects of their change ideas had not yet been ‘Implemented’, that is, they had not taken all the actions necessary to sustain the gains described in these resources. The team also knew that the service was in the process of undergoing some redesign in terms of the role of community and inpatient consultant psychiatrists. Based on these factors, their prediction was that the gains would not be sustained and further testing might be necessary to respond to these factors. They kept the project open while they continued to monitor the data. As the chart shows, their prediction was realised in July and August 2016 when the average bed occupancy went up to 77%. When this happened, they did not introduce new change ideas, but ran further PDSA cycles (Plan do Study Act) to refine and improve the existing change ideas that had previously proved successful. This allowed them to bring the performance back under control.

Figure 1. Bed Occupancy displayed on a P Chart (percentage)
In summary, if your project has achieved its improvement aim and you have successfully undertaken the implementation tasks and testing, you can close the QI project as ‘complete’. You should however have a plan for quality control, that is, a plan of how you will maintain control within agreed parameters of what is expected in the new system. You can also set thresholds identifying exceptions and how to escalate this. When this happens a decision may be made about how to understand the exception and how to respond to it. A typical approach would be to analyse the process to see if it’s operating reliably to produce the results you expect. If it is not, you may look at testing some change ideas using PDSA cycles to try and address the issue. It is up to the subject matter experts to decide whether this will be done through a formal QI project or not. Once the issue is resolved through PDSA cycles and improved design, you can revert back to quality control. This relationship between Quality Improvement and Quality Control is well illustrated in figure 2 below.
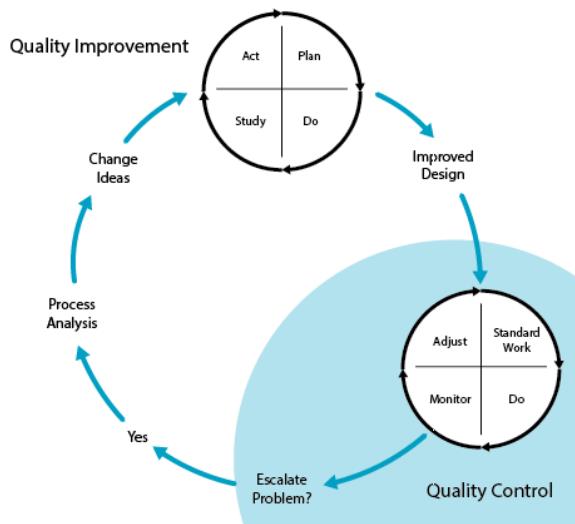
Figure 2. The relationship of quality improvement and quality control
You can read more about sustaining improvement in the white paper by the IHI available here: http://www.ihi.org/resources/Pages/IHIWhitePapers/Sustaining-Improvement.aspx
Most Read Stories
-
Why is Quality Control important?
18th July 2018

-
2016 QI Conference Poster Presentations
22nd March 2016
-
Recognising Racism: Using QI to Help Take Action
21st January 2021

-
QI Essentials: What does a Chief Quality Officer do?
18th March 2019

-
-
Using data enabled us to understand our problem
31st March 2023


Follow QI on social media
To keep up to date on the latest concerning QI at ELFT, follow us on our socials.
